

Shared with permission from UTT BioPharma
Written by: Abdul Rehman Mohammad
Playing a role in almost every physiological system in the body, the endocannabinoid system is a key homeostatic regulator. Historically it has been overlooked as a possible therapeutic target, as there was not much known about disease implications of the system. However with the incredible success stories reported from the use of cannabidiol (CBD) and cannabidiolic acid (CBDA), the endocannabinoid system is increasingly gathering interest in the medical community.
The theory of clinical endocannabinoid deficiency is progressively gathering supportive evidence for it’s involvement in migraine, fibromyalgia and irritable bowel syndrome. Some diseases have shown endocannabinoid abnormalities such as epilepsy, cancer and a wide array of neurodegenerative diseases.
CBD and CBDA have shown to be very effective at treating a variety of conditions, and their therapeutic evidence and value is growing daily. The precise mechanism of action for both of these compounds is still debated. However by inferring from their pharmacological characteristics, conclusions can be drawn on the diseases which would benefit the most from these compounds.
Cannabidiol: how does it work?
CBD has very little action at the CB1 and CB2 receptors. It is able to block the actions of compounds which activate these receptors, such as THC. Consequently it can suppress that psychoactivity of THC, and can be effective to reduce it’s side effects.
CBD also inhibits the enzyme which degrades anandamide, fatty acid amide hydrolase (FAAH), and can consequently restore anandamide levels in diseases which have shown clinical endocannabinoid deficiency. A clinical study using CBD for schizophrenia brought about a significant increase in serum anandamide levels, consequently bringing about a marked clinical improvement.
The chemical structure of cannabidiol (CBD)
As CBD is an enantiomeric compound, it’s different enantiomers can have varying effects. A study has shown that the (−)-enantiomer was better at inhibiting FAAH as compared to the (+)-enantiomer. In contrast, the (+)-enantiomer showed more affinity for the CB1 and CB2 receptors and would probably be a better compound to be given in combination with THC.
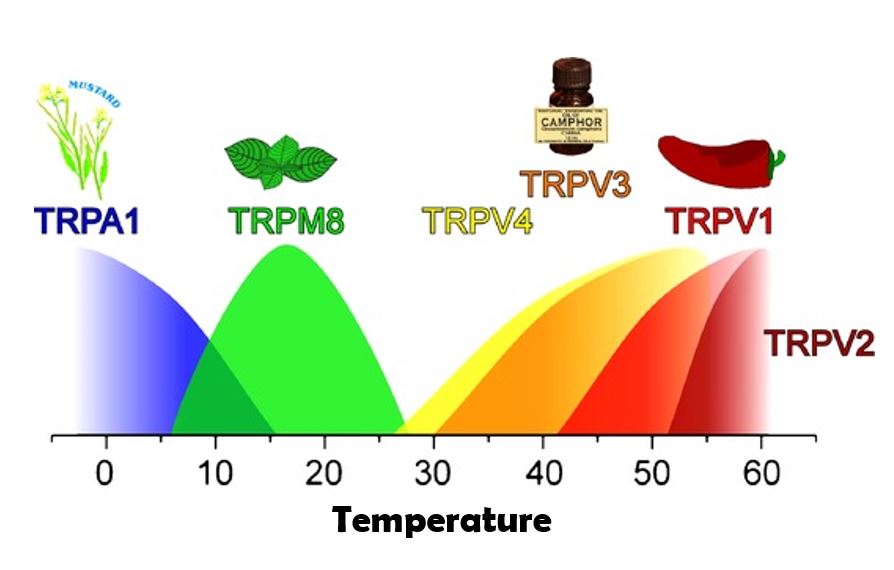
CBD also has affinity at certain Transient receptor potential (TRP) cation channels, which are implicated in many diseases. CBD desensitizes (dampen the receptor’s activity) TRPV1, TRPV2, TRPV3, TRPV4 and TRPA1 channels which are highly active in pain states in many diseases. CBD is also an antagonist of the TRPM8 receptor, which heavily implicated in allodynia. CBD also targets key neural signalling receptors such as 5-HT1a and 5-HT3a, which are useful targets for diseases such as epilepsy and numerous anxiety disorders.
Cannabidiolic acid: the precursor with an important role
A heat activated reaction causes the removal of the carboxyl group on CBDA, and leads to the formation of CBD. CBDA’s interaction with the endocannabinoid system is minimal, but it has other interesting target receptors. CBDA desensitizes the TRPV1, TRPV3, TRPV4 and TRPA1 receptors. CBDA also inhibits key inflammatory mediators such as COX-1 and COX-2.
The COX-1 enzyme is a promising target for reducing seizures, and the use of CBDA in the treatment of epilepsy has been patented by British company GW Pharmaceuticals. COX-2 is responsible for a wide range of inflammatory processes in the body. Other well known COX-2 inhibitors include acetylsalicylic acid (Aspirin), naproxen, ibuprofen and tolmetin. CBDA could mimic the effects of these drugs in treating inflammation.
Working in synergy
Diseases are often caused by the misregulation of multiple physiological systems in the body. As suggested by anecdotes, the combination of CBD and CBDA could be much more effective than the single compounds, especially for diseases such as epilepsy. By complementing each other’s properties, they could work very effectively. Recently published data has revealed that acidic cannabinoids (such as CBDA) can help the uptake and metabolism of CBD or other phytocannabinoids. Administering CBDA with CBD could decrease the amount of CBD needed to be effective.